Gene Therapy for Climbers?
Sherpas' high-altitude endurance owes a lot to denser capillaries and better microcirculation, not just thicker blood. Could VEGF gene therapy reproduce that capillarization in lowland climbers?
Recently, a story from Everest happened that sounds almost unbelievable. Dawa Sherpa, a 52-year-old mountain guide, went missing on the mountain and was found alive about a week later: he was discovered crawling down snowy slopes; he had spent almost a week without food, water, or supplemental oxygen. These are conditions in which most lowland climbers would rarely survive even one night.
Sherpas are an ethnic group living in the mountains of Nepal and known for remarkable endurance in the mountains. As a result, many of them work on Everest and other mountains. When an ordinary lowland climber performs a feat, climbs Everest, and posts summit photos, you should know that a Sherpa usually went up in parallel, often carrying equipment both for himself and for the lowland climber, and sometimes the lowland climber too.
Moreover, many climbers somehow perceive Sherpas almost like mutants on doping, whose achievements do not count.
The first confirmed ascent of Everest was on May 29, 1953. In popular memory, most of the glory went to Edmund Hillary. But the person who reached the summit with him was Sherpa Tenzing Norgay, whose name is far less widely known.
They reached it together. Hillary probably chose a Sherpa partner for a reason: a lot of difficult work was likely done by Tenzing as well. Technically, Hillary stepped onto the summit first, because Tenzing was a hired worker in that expedition.
After the success of 1953, Hillary and expedition leader John Hunt were knighted. Tenzing Norgay received the George Medal, and for some reason he was not knighted.
This is how Sherpas have often been treated throughout the history of mountaineering. As genetically different people whose achievements somehow don’t count: as if they are so biologically separate that there is no point for a lowlander even trying to compete with them. But now we live in an amazing time: we have biotech. We can understand the secret of Sherpa endurance and, possibly, create a therapy that could help level the endurance gap between lowland climbers and Sherpas.
Why the mountains are so hard
Climbers have a hard time in the mountains not because “there is less oxygen in the air as a percentage”: oxygen is still about 21%. The problem is that atmospheric pressure falls, the air becomes thinner, and with each breath fewer oxygen molecules enter the lungs.
In the Xtreme Everest microcirculation study, measured barometric pressure was about 100.6 kPa in London at 35 m, but about 53.0 kPa at Everest Base Camp at 5300 m. The calculated partial pressure of oxygen fell from 21.0 kPa to 11.0 kPa. In other words, the oxygen percentage barely changes, but the pressure driving oxygen into blood and tissues is almost cut in half.
At altitude, the body switches into a struggle-for-oxygen mode. Breathing becomes faster and deeper, the heart beats faster, blood is pumped more intensely, but it is still not enough. Muscles cannot produce energy normally, so steps become shorter, every movement feels like too much effort, and climbing a slope feels like running at your limit. The brain also suffers: thinking slows, coordination, memory, self-control, and decision-making get worse. That is why at high altitude a person can make dangerous mistakes even if he is experienced and well prepared.
Everest is especially hard because of the “death zone”, usually heights above about 8000 meters. At around 5000 m the atmosphere contains roughly half the oxygen pressure compared with sea level; at 7000 m clear thinking becomes difficult; and at 8000 m even the strongest climbers can survive only for a limited time. In a study of arterial blood gases in Everest climbers, researchers measured extremely low arterial oxygen levels at extreme altitude; this shows how close to the limit the body is working there.
As a result, many people think that the best organism is the one that makes more hemoglobin and red blood cells. But for Sherpas it is more subtle. Their adaptation is not reduced to thick blood. On the contrary, one feature of Tibetan-Sherpa high-altitude populations is a more moderate hemoglobin response to hypoxia.
Put simply, the Sherpa strategy is not just “carry more oxygen in the blood.” Their advantage is to deliver oxygen to tissues and use it more efficiently.
And this is where it becomes most interesting for climbers.
The bottleneck: capillaries
The bottleneck of oxygen delivery is capillaries. The better the capillary network, the shorter the distance from blood to mitochondria, the larger the exchange surface, and the better tissues receive oxygen and remove metabolic byproducts.
This is exactly where Sherpas show one of the most interesting features. In the Xtreme Everest microcirculation study, researchers compared 64 Sherpas with 69 lowlanders. The lowlanders were recruited in the UK, were not descendants of native high-altitude populations, and were born and lived below 1000 m. The groups followed an identical ascent profile to Everest Base Camp, and the researchers imaged sublingual microcirculation using incident dark field imaging.
At about 5300 m, Sherpas had higher microcirculatory blood flow, more homogeneous flow distribution, and higher small-vessel density. In some measurements, capillary density in Sherpas at altitude was up to 30% higher than in lowlanders.
Specifically, at Everest Base Camp, small-vessel microvascular flow index was higher in Sherpas than in lowlanders: 3.00 vs. 2.66. Small-vessel density was also higher: 13.83 vs. 10.52 mm/mm².
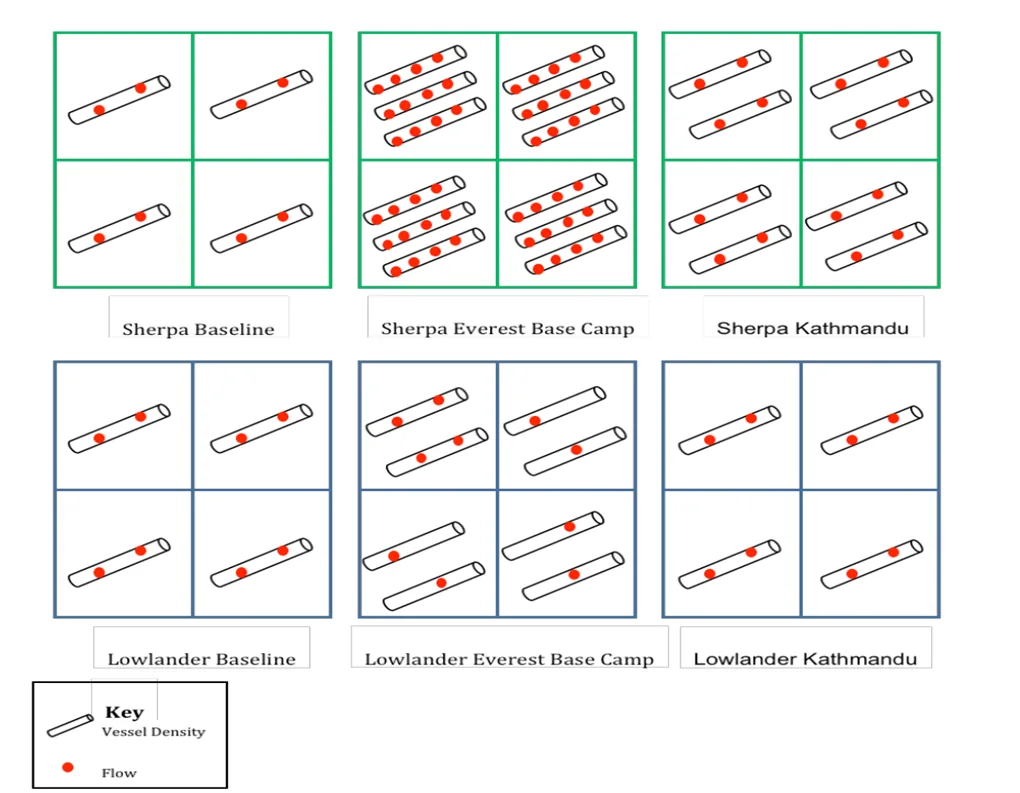
Figure 1. Original schematic from Gilbert-Kawai et al., Journal of Applied Physiology, 2017. The white vessel icons visualize small-vessel density, and the red dots visualize microvascular blood flow. At Everest Base Camp (middle panels), Sherpas show both denser small vessels and greater flow than at baseline, whereas lowlanders show only a modest increase in vessel density together with sparser, less uniform flow. This visual pattern matches the quantitative results discussed in the text: at Everest Base Camp, the small-vessel microvascular flow index was 3.00 in Sherpas vs 2.66 in lowlanders, and small-vessel density was 13.83 vs 10.52 mm/mm².
Sherpa endurance is not related to the fact that they “heroically endure” hypoxia, but to the fact that their tissues may actually be supplied with oxygen better at the microcirculation level.
If capillaries are one of the key elements of Sherpa adaptation, a logical hypothesis emerges: could we artificially enhance capillarization in an ordinary lowland climber with VEGF gene therapy and thereby bring him closer to one component of Sherpa endurance?
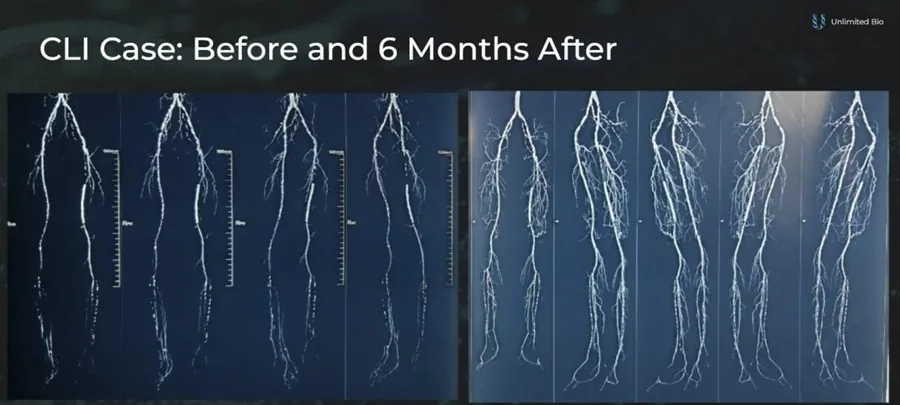
Building a new capillary network in a critical limb ischemia patient (Stage IIb) with VEGF gene therapy. Source: Unlimited Bio
This hypothesis rests on three blocks of data.
First: at altitude, Sherpas really do have better-functioning microcirculation and higher small-vessel density.
Second: muscle capillarization is a proven adaptive mechanism of endurance training. A review of muscle capillarization says training can increase the number of capillaries per muscle fiber by about 10-20% within several weeks in untrained people, and capillarization itself affects oxygen diffusion conditions.
Third: VEGF is a central regulator of capillary growth. Experimental work showed that without VEGF produced by muscle cells, normal capillary adaptation of skeletal muscle to training does not occur.
Conclusion
Sherpas are not mutants and not “mountain robots.” They are people whose biology is better adapted to life and work where oxygen is scarce. Their advantage comes from hypoxia-response genes, features of blood, vessels, capillaries, muscle energetics, childhood at altitude, training, and the culture of mountain work.
The story of Dawa Sherpa shows how far human survival can go in conditions where ordinary physiology breaks down. The story of Tenzing Norgay reminds us that from the very beginning Sherpas were not the background of great ascents, but their equal participants.
If we are looking for a biological mechanism that could be at least partially reproduced in climbers, capillarization is one of the most logical candidates.
VEGF gene therapy could theoretically become a tool to test this.
Do you know anyone preparing for Everest? Let’s talk :)
References
-
Reuters. Sherpa rescued after going missing on Everest with no food, oxygen. https://www.reuters.org/world/asia-pacific/sherpa-rescued-after-going-missing-everest-with-no-food-oxygen-2026-06-04/
-
History.com. Edmund Hillary and Tenzing Norgay reach the Everest summit. https://www.history.com/this-day-in-history/may-29/hillary-and-tenzing-reach-everest-summit
-
The Guardian. Everest anniversary: Tenzing Norgay’s grandson calls for ‘gesture’ from Britain. https://www.theguardian.com/world/2013/may/29/everest-anniversary-tenzing-norgay
-
Grocott MPW, et al. Arterial blood gases and oxygen content in climbers on Mount Everest. N Engl J Med. 2009. https://www.nejm.org/doi/full/10.1056/NEJMoa0801581
-
Gilbert-Kawai E, et al. Sublingual microcirculatory blood flow and vessel density in Sherpas at high altitude. J Appl Physiol. 2017. https://pmc.ncbi.nlm.nih.gov/articles/PMC5407196/
-
Peripheral limitations for performance: muscle capillarization. https://pubmed.ncbi.nlm.nih.gov/37770233/
-
Olfert IM, et al. Myocyte vascular endothelial growth factor is required for exercise-induced skeletal muscle angiogenesis. https://pmc.ncbi.nlm.nih.gov/articles/PMC2957383/
-
Population history and altitude-related adaptation in the Sherpa. Front Physiol. 2019. https://www.frontiersin.org/journals/physiology/articles/10.3390/fphys.2019.01116/full